The misnamed "Spanish Flu" pandemic peaked in late 1918 and remains the most widespread and lethal outbreak of disease to afflict humankind worldwide in recorded history. (Note: In September 2021 it was announced that Covid-19 had killed more Americans than the Spanish Flu, 681,000 vs. approximately 675,000. However, the U.S. population is now three times greater than it was in 1918, and in percentage terms the Spanish Flu was considerably more lethal. As of December 2021, Covid-19 had taken the lives of approximately 5.25 million people worldwide. Estimates of the global death toll from the Spanish Flu, when accurate record-keeping was a rarity, range from an unrealistic minimum of 20 million to as many as 100 million.) In the earlier pandemic, small mutations in a flu virus created an extraordinarily lethal variant that killed healthy young adults as readily it did more vulnerable age groups. The pathogen's place of origin is still debated, but the role of World War I in its rapid spread is undisputed. Even so, Washington state, despite a heavy military presence, fared better than any other state in the union except Oregon. While the death toll was highest in our most populous cities, the pandemic touched nearly every community. Attempts to control the outbreak were largely futile, and from late September 1918 through the end of that year it killed nearly 5,000 Washingtonians. More than half the victims were between the ages of 20 and 49.
An Ancient Scourge
Influenza viruses probably first sickened humans 6,000 to 7,000 years ago, corresponding with the early domestication of pigs and cattle. Increased human mobility facilitated epidemics and pandemics that could affect vast areas. Until the early 1930s influenza was thought by most scientists to be a bacterial rather than a viral disease. In fact both were often involved; those weakened by an influenza virus were left more vulnerable to bacterial pneumonia. Still, during flu's annual visitations it usually caused only moderate illness. But now and then something different and far more lethal came along.
The first recorded pandemic likely caused by an influenza virus came in 1580 and ravaged an area stretching from Asia Minor to as far north as today's Netherlands. There were frequent large outbreaks thereafter, but relatively few deaths. A more lethal virus struck Europe and the Russian empire in 1781-1782, and in 1889 and 1890 more than a million people died when a deadly variant burst from China, spread to Russia and throughout Europe, and made its way to North America and Latin America before sputtering out in Japan. Next came the pandemic of 1918, by far the most widespread and deadly, a dismal distinction that stands to the present day.
American Samoa was the only organized society on the planet to entirely escape the 1918 pandemic, thanks to an early, rigorous, and lengthy quarantine. In Western Samoa, barely 50 miles distant, 20 percent of the population died in a matter of months. Flu girdled the globe from east to west and from north of the Arctic Circle to the southern tip of Chile, leaving in its wake shattered societies and tens of millions dead.
A Different Disease Entirely
Before 1918 the average mortality rate for most influenza was only about one-tenth of 1 percent, or approximately one fatality for every 1,000 infections. The 1918 flu killed more than 2.5 percent of those afflicted, almost always within days of the first symptoms and often within hours. Some died from acute respiratory distress (a direct effect of the flu virus) and others fell prey to opportunistic bacterial pneumonia. And unlike almost any previous known infectious disease, this virus hit adults between ages 20 and 40 particularly hard.
World War I was in its final months when the worst of the pandemic hit. Approximately 53,500 Americans lost their lives in combat and a nearly equal number died of influenza while serving in Europe. The number of Americans, military and civilian alike, killed by the virus back home was estimated to be in excess of 650,000. The most conservative (and perhaps least accurate) estimate of the death toll worldwide is more than 20 million, and as many as 100 million may have died (many governments kept few or no accurate records, making even rough estimates highly problematic).
American Flu?
It's unknown where the pandemic originated. It was commonly called the "Spanish flu," probably because Spain, which didn't participate in World War I, freely reported illnesses and deaths caused by the disease, information that was censored by the combatant nations. The prejudiced suspicion that deadly infectious diseases spring from rural pig sties in Asia or the steamy jungles of sub-Saharan Africa probably was not true in 1918. One supportable theory holds that the "Spanish" flu originated in Haskell County, Kansas, where in February 1918 a local doctor was overwhelmed by a number of cases of a particularly virulent and deadly illness, unlike anything he had seen in long years of practice. During the outbreak a local man came home on leave from the army, then returned to Camp Funston in the sprawling Fort Riley complex 300 miles away. Within three weeks, more than 1,100 soldiers at the camp were hospitalized with the flu and 28 did not survive, an unusually high mortality.
By early April significant outbreaks of a milder flu were reported, including in Detroit, where as many as 2,000 workers at the Ford automobile plant were stricken. The deadly variant hit Spain in late May. The mystery remains today -- it is uncertain where the "normal" flu virus mutated into an efficient killer. Competing theories range from Kansas to Norway to English Channel ports to the usual suspect, China. It is unlikely that this question can ever be conclusively resolved, and it hardly matters.
One fact is undisputed: War and disease went hand in hand. During the spring of 1918, convoys were carrying American troops to fight in World War I and returning with wounded, ill, and demobilized soldiers. While the conflict apparently had no direct link to the origins of the virus, it had everything to do with its spread.
Hints of a Coming Cataclysm
Many of the cases reported in the middle months of 1918 were relatively mild and localized, but in late August events took a dire turn when the deadly variant broke loose:
"It occurred in three major parts of the North Atlantic almost simultaneously: Freetown, Sierra Leone, where local West Africans were brought together with British, South African, East African, and Australian soldiers and sailors; Brest, France, which was the chief port for Allied troops; and Boston, Massachusetts, one of America’s busiest embarkation ports and a major crossroads for military and civilian personnel of every nation involved with the Allied war effort. Massive troop movements and the disruption of significant segments of the population during World War I played an important role in the transmission of the disease" ("Influenza," Medical Ecology website).
In Washington the first eight months of 1918 seemed similar to most years, and newspapers in the state apparently took no notice of spring outbreaks of flu in Detroit and a few other American cities. On April 15, however, it was reported that at the army's Camp Lewis south of Tacoma, "Pneumonia has slightly increased during the week, most of the cases follow influenza, which was at its maximum two weeks ago" ("Civilian Workers Fast Being Eliminated ..."). In late May The Seattle Times carried a brief wire-service report stating that "a mysterious epidemic" had sickened at least 40 percent of Spain's population, and that although the symptoms "resemble influenza ... many persons afflicted with it have fallen in the streets in a fit" ("Unknown Disease ... "). One week later, the paper said of the Spanish outbreak, "The rapidity of its spread is comparable only to the great plague of 1889," a reference to the flu pandemic of nearly 30 years before ("King Visited by Strange Illness"). In June there were gleeful reports of a flu epidemic among enemy German soldiers, but early that month Camp Lewis reported just 39 cases.
Things seemed more ominous by early July. On July 9, The Seattle Times reported that the influenza in Spain had "spread over other parts of Europe" ("A Puzzling Epidemic"). On July 28 the newspaper noted that Camp Lewis had 327 cases of flu, but a week later the number had fallen to below 100. As late as mid-August there were reassuring reports that the count of flu cases at the army base continued to decrease, and no indication of any special concern. Even into September, the general mood was one of confidence. An optimistic commentator enthused, "It is a marvel, due to the perfection of our medical science, that there has been no widespread epidemic this summer of a more serious character than 'flu,' as the Spanish influenza and other allied fevers are called" ("Heavy Rain and Mud ... ").
As the month wore on, a tone of modest alarm began to creep into some accounts. A Times article on September 22 referred to a "mild epidemic" at Camp Lewis, with 173 new cases reported ("Camp Lewis Reports ... "). On the same page, mention was made of two serious cases of influenza reported in Bellingham. Still, two days later army medical sources were quoted in the newspaper as saying, with some jocularity, "There may have been a Spaniard with influenza at Camp Lewis, but there is no Spanish influenza here" ("Say Camp Lewis ... ")..
This could have been whistling past the graveyard, but in truth no one had any understanding of the tsunami that was building. What was happening was not remotely within the knowledge of the brightest scientists and doctors of the era. The virus that caused influenza had mutated, and in ways that would make it one of the most deadly pathogens to ever afflict the human race. When it fully hit America it moved with breathtaking speed through the entire country, helped at every turn by a war-mobilized military.
Spreading Like Wildfire
Between September 1918 and the war's end in November, up to 40 percent of American army and navy personnel were infected with influenza. The nexus between the military and the rapid spread of the pandemic was starkly clear. State health officials were aware of the danger. The minutes of a state Board of Health meeting in Spokane on September 28, 1918, noted, "The probability of an outbreak of influenza in the State was extensively discussed and ways and means of attempting its prevention were considered" (Twelfth Biennial Report, 6).
It would prove to be both unpreventable and essentially untreatable. Just two days later, on September 30, at the University of Washington Naval Training Station on Seattle's Portage Bay (the current site of the university's Health Sciences complex), more than 650 cases of "mild influenza" were reported ("Navy Camp at 'U' ... "). In the first week of October more than 100 cases of "severe influenza" were documented at Camp Lewis. Cases were also found at the Puget Sound Naval Shipyard in Bremerton, and on October 4 it was reported that 14 naval recruits had died there and "between 200 and 400" civilian workers at the navy yard had become ill ("Bremerton Hit ... "). These reports were harbingers of much worse to come as the deadly virus spread with amazing speed.
A Dearth of Data
For several reasons, tracking the progress of the pandemic in the state with much accuracy is impossible. First, influenza was not a disease that had to be reported to state health authorities, at least not during its most virulent phase in the fall of 1918. Voluntary reporting was extremely sporadic, as will be seen. Deaths needed no diagnosis and were faithfully recorded, but overall tallies of the infected must be considered rough estimates, even when impressively specific.
Second, the flu in 1918 and early 1919 came in three distinct waves -- a usually mild form in the spring and summer of 1918, followed by the deadly strain in the closing months of that year, and ending with a return of usually (but not always) milder disease in the early months of 1919 , not fully tapering off until 1920. Not everyone who became ill was infected with the virulent "Spanish" flu; some had a more mild form, which still could be lethal to the very young and the elderly.
To further frustrate public-health authorities, the Spanish flu killed both directly and by leaving victims vulnerable to secondary infections with bacterial pneumonia, which was often fatal even in the absence of the flu, particularly in the elderly or infirm. This muddled the causality picture. But because the Spanish flu had proven so stunningly contagious and pneumonia was so often found during autopsies of flu victims, the federal Census Bureau decided to use a single category in its mortality statistics for 1918: "deaths from influenza and pneumonia (all forms)" (Mortality Statistics, 1918). As frustrating as it is to epidemiologists and life-insurance actuaries, all statistical studies of the effects of the 1918 pandemic are riddled with uncertainty and approximations.
What the Record Shows
Washington was one of 30 "registration states" deemed by the U.S. Census Bureau to have reasonably reliable recordkeeping in 1918, but the state's epidemiologist, in a January 1919 Board of Health biennial report to Governor Ernest Lister (1870-1919), emphasized the unprecedented nature of the pandemic and the difficulty of gathering accurate information:
"This pandemic made its appearance in Washington in the first week of October. In the history of the State Board of Health no such calamity has afflicted the State nor has so serious an emergency ever arisen. In the five years 1913-1917 inclusive, from the five most common contagious diseases ... there have been 1768 deaths. From influenza alone we have had to date well over 2000 deaths and the end is not yet. The toll will probably be double or triple 1768 ... .
"City health officers, except in Seattle, Tacoma, Spokane and Yakima, are part-time men. Their salary is often nothing or five dollars a month. They are appointed by their mayors and change frequently. They are not of our making and do not feel as if they have much responsibility to us. Their jobs pay little and their policy is to do as much as the pay justifies" (Twelfth Biennial Report, 34-35).
The report was prepared in December 1918, when the full extent of the catastrophe was unknown. The health board's next biennial report was not issued until January 1921 and was almost silent on the 1918 pandemic. There appears to be no available compilation, state or federal, of infection rates or deaths on a county-by-county basis, much less for individual communities, although census data does exist for Washington's two largest cities, Seattle and Spokane, and Yakima's experience is relatively well documented.
In its Mortality Statistics 1918 the U.S. Census Bureau compared the state's total 1918 flu deaths with those from 1915, contrasting the first eight months of each year with the last four. Between January and August of 1915, 605 Washington residents died of influenza and pneumonia; in the first eight months of 1918, 838 Washingtonians died, a sizable but not shocking increase.
In the last four months of 1915, only 381 people in Washington succumbed to the flu, but in the last four months of 1918, the pandemic killed 4,041 in the state, 10.6 times the 1915 count for the same period. The state epidemiologist's pessimism about the final toll proved fairly accurate.
Other facts from the mortality tables demonstrate the unprecedented nature of the Spanish flu. Perhaps most surprising, slightly more than half, or 2,461 of the 4,879 flu fatalities in Washington in calendar year 1918, were men and women between the ages of 20 and 39, the demographic group that normally enjoyed the highest disease survivability. The same rough proportions held true in the state's two largest cities. In Seattle 708 of 1,441 flu deaths recorded between October 12, 1918, and March 15, 1919, fell into that age range, while in Spokane the count was 252 of the 428 flu deaths. These numbers alone illustrate just how unique this pandemic was in comparison to any other disease outbreaks for which records exist. This mystery has never been fully resolved, but the leading theory is that the 1918 virus triggered catastrophic immune reactions in young adults with robust immune systems.
Comparative numbers were not calculated for Yakima, but roughly one-third of the population, or about 6,000 people, were infected there. Of these, 120 died -- 32 percent of the city's total 1918 death toll from all causes. So contagious was the disease that Yakima's only hospital, St. Elizabeth, run by the Sisters of Providence, for a time refused to admit influenza patients.
There is only one statistic in the 1918 mortality tables from which some comfort may be taken. Of the 30 registration states relied upon by the Census Bureau, with the single exception of Oregon, Washington by a significant margin had the lowest number of influenza/pneumonia deaths per 1,000 residents. Nevertheless, 4.1 of every 1,000 Washingtonians were killed by influenza/pneumonia in 1918 (more than five times normal) and 1.9 of every 1,000 in 1919 (more than twice normal). In contrast, the state's mortality rate from those causes in each of the three preceding years was less than one per 1,000.
Doing Their Best
The health board's Twelfth Biennial Report documented both a realistic apprehension of the danger Spanish influenza presented and a recognition of the futility of efforts to prevent it. It recounted the efforts of Dr. Thomas D. Tuttle, the state's health commissioner and the report's lead author, to get advice from the federal government:
"This epidemic was very prevalent in the Eastern states during the month of September, and, realizing that in all human probability it would rapidly spread over the entire country, your commissioner of health took up with the United States Public Health Service the question of the advisability of quarantining individual cases" (Twelfth Biennial Report, 22-23).
Specifically, the board reported, Tuttle sent a telegram to U.S. Surgeon General Rupert Blue asking "Intrastate quarantine Spanish influenza under consideration. What period of quarantine if any do you recommend?" and Blue relied "Service does not recommend quarantine against influenza" (Twelfth Biennial Report, 22-23).
In the report Tuttle provided the health board's opinion on how the Spanish flu came to Washington. It is but one theory among several, but as credible as any:
"The epidemic struck our state in the early part of October. The immediate introduction of the disease was through a shipment from Pennsylvania to the United States Naval Training Station at Bremerton of about 1500 men, a large percentage of whom were afflicted with influenza when they reached their destination. From this location the disease spread widely [but] many outbreaks were not directly traceable to the infection at or near Seattle" (Twelfth Biennial Report, 23).
Tuttle's account of a Chicago meeting of state health authorities could not conceal a tone of desperation:
"The outstanding feature of the discussion of the subject at this conference was the evidence that whatever efforts were made the spread of the disease was only retarded and not prevented. As one health officer very aptly expressed the situation: 'One can avoid contracting the disease if he will go into a hole and stay there, but the question is how long he would he have to stay there? The indications are that it would be at least for a year or longer'" (Twelfth Biennial Report, 23).
Desperate Measures, Mostly Futile
Despite its early concerns, the Washington State Board of Health did not impose statewide measures to combat the pandemic until it was well under way, probably because it had very limited resources and little or no control over local health authorities. The only preventive regulation of statewide application that the board issued came on November 3, 1918, when it required that surgical masks of a specified size and thickness "entirely covering the nose and mouth" be worn in virtually all public places where people came into close contact with one another; the order also required that the proprietors of stores, restaurants, and cafes "keep their doors open and their places well ventilated" and that one-third of the windows in streetcars be opened when in use by the public ("Special Order and Regulation ... ").
Vancouver in Clark County was one of the first cities in the state to aggressively address the pandemic. On October 7, 1918, acting on a report from the chief health officer, the city council ordered that "all places of public gathering, such as schools, churches, dances etc." be closed (Vancouver City Council minutes). Two days later the town council of Monroe in Snohomish County approved a similar measure, as did Yakima, which later joined with Yakima County to lease a building owned by St. Michael's Parish "for the purpose of establishing same as an Isolation Hospital" (Yakima City Commission minutes, October 21). On October 31 the ban on gatherings in Yakima was widened even further to include "all places where any kind of business is transacted ... with the exception of drug stores, meat markets, restaurants, eating places, hotels and fruit ware-houses," the last an apparent concession to the town's leading industry (Yakima City Commission Minutes, October 31).
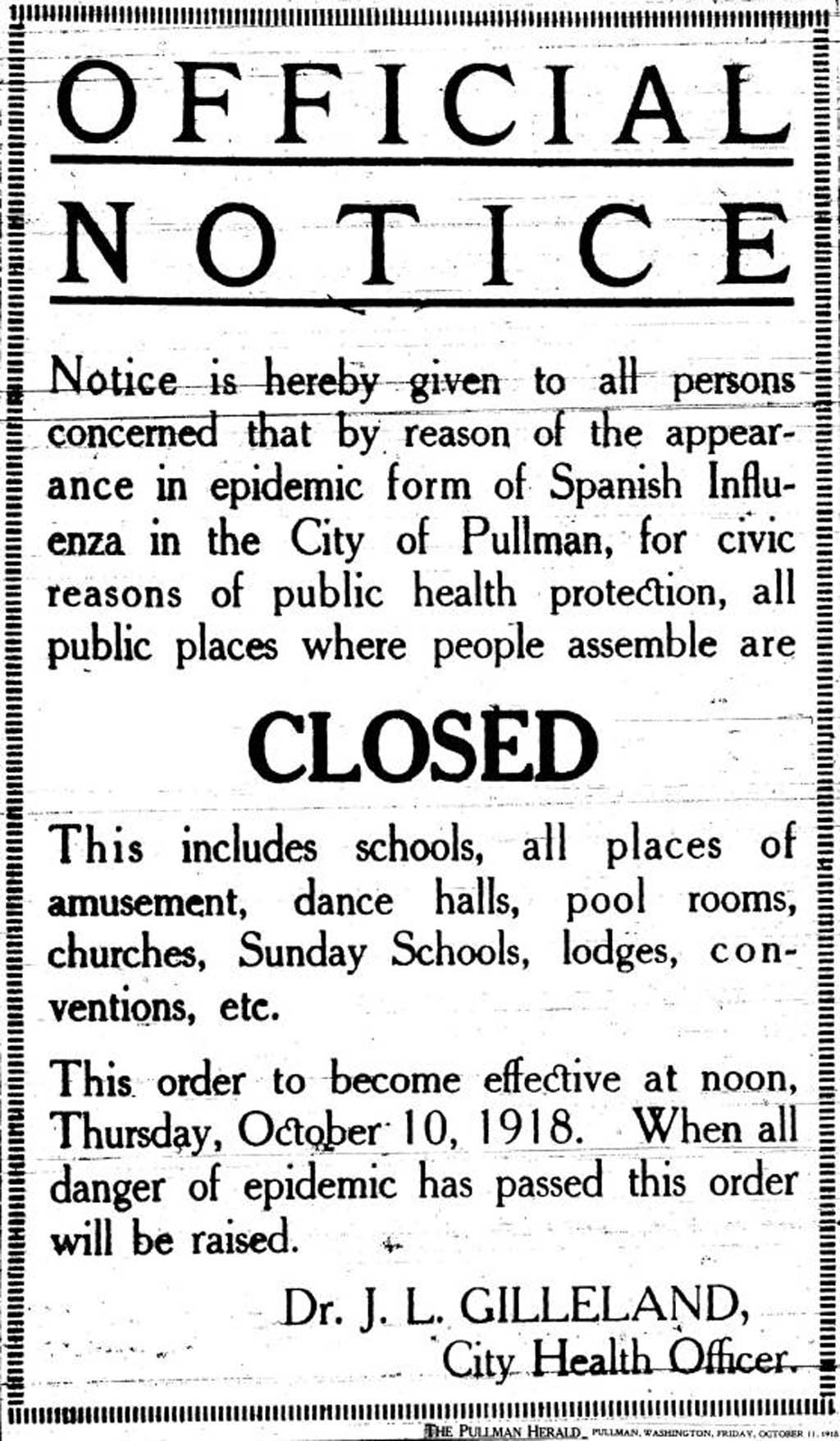
Similar bans on public assembly were imposed in counties, cities, and towns across the state. A small sample would include Seattle (October 6); Spokane (October 8); Pullman (October 10); Anacortes in Skagit County (October 15); Ferry County in Northeast Washington (November 17); tiny Wilson Creek in Grant County, where all children under age 16 were ordered confined to their homes (December 7); and Chelan, although it exempted schools (December 10). No corner of the state was spared, nor did the ordeal end with the new year. The Cowlitz County Council did not even impose similar restrictions until January 16, 1919, and White Salmon to the east was at that time still under siege.
These and similar measures probably helped to limit the spread to some extent, but perhaps the most telling reason for the eventual ebbing of the pandemic was that it simply ran out of vulnerable victims. In this regard it is important to remember that most people did not become infected, despite nearly universal exposure, nor did it kill but a fraction of those it did infect.
What Was It? Where Did It Go?
In the 1990s researchers, using archived autopsy samples from 1918, mapped the virus's genome and determined it to be Type A, the most common, which can infect both humans and some animals. More specifically, the investigation revealed that the virus was a strain of Type A known as H1N1. The "H" represents a protein molecule on the surface of a virus that is the usual target for the immune system. When random mutations alter that molecule, the virus can become virtually invisible to the body's defenses. As researchers explained in 2006, "Recently published ... analyses suggest that the genes encoding surface proteins of the 1918 virus were derived from an avianlike influenza virus shortly before the start of the pandemic and that the precursor virus had not circulated widely in humans or swine in the few decades before" (Taubenberger and Morens, 16). Because it had not circulated widely, humanity had developed no "herd immunity" to it. This explains its rapid spread but not its lethality, which remains a mystery.
As to where it went, the answer is that it went nowhere. Almost all cases of type A influenza since 1918 have been caused by less-dangerous descendants of that lethal virus. Viruses do not have intentions, only random mutations. Some mutations will enable them to sicken birds, pigs, people, or other animals. Some will make them unusually lethal, others will render them totally harmless to humans. But inevitably a strain will emerge that is as infectious and deadly as the 1918 variety. Viral mutation is ongoing, endless, and unpredictable. In any new flu pandemic the toll will likely be lower due to advances in immunology and other countermeasures, but as with death itself, the question is not whether it will come, but rather when.